Indian Journal of Physiology
and Pharmacology
and Pharmacology
Indian Journal of Physiology and Pharmacology |
 (252x320).jpg) |
Volume 58 - Number 2 April - 2014 (Current issue) ISSN 0019-5499 |
Effect of Rajyoga Meditation on Chronic Tension HeadacheKiran, Kawalinder K Girgla, Harsh Chalana and Harjot Singh |
Chronic tension-type headache (CTTH) is the most common type of headache with no truly effective treatment. This study was designed to correlate the additive effect of meditation on CTTH patients receiving medical treatment. 50 patients (aged 18-58 years) presenting with a clinical diagnosis of CCTH, were divided in 2 groups.Group 1 (n=30) received 8 lessons and practical demonstration of Brahmakumaris spiritual based meditation known as Rajyoga meditation for relaxation therapy, in addition to routine medical treatment (analgesics and muscle relaxants). Group 2 (n=20) patients received analgesics and muscle relaxants twice a day but no relaxation therapy in the form of meditation. Both groups were followed up for 8 weeks period. The parameters studied were severity, frequency and duration of CCTH, and their headache index calculated. Patients in both groups showed a highly significant reduction in headache variables (P<0.001) after 8 weeks. But the percentage of patients showing highly significant relief in severity of headache, duration & frequency in Group 1 was 94%, 91% and 97% respectively whereas in Group 2 it was 36%, 36% and 49% respectively. Headache relief as calculated by headache index was 99% in Group 1 as compared to 51% in Group 2. Even Short term spiritual based relaxation therapy (Rajyoga meditation) was highly effective in causing earlier relief in chronic tension headache as measured by headache parameter. |
Headache is an almost universal experience. Tension type is the most common type of headache with global prevalence of 42% (1). The International Headache Society recognised that in chronic tension type headache (CTTH) there are 15 or more headache days per month. This division of tension headache into episodic and chronic is arbitrary and is based upon clinical observations that CTTH is difficult to treat (2). All variety of drugs and physical therapy and their combinations are commonly prescribed to these patients but their efficacy is controversial (3). Various psychosocial and other mind-body approaches used for relieving pain and relaxation are diaphragmatic breathing, deep muscle relaxation, selfhypnosis and autogenic techniques like biofeedback, yoga and meditation (4). Relaxation of body, mind and behavioural change with positive approach has been successfully achieved by Rajyoga meditation (5). Rajyoga meditation of the Brahmakumaris is a
behavioural intervention, with the organization's
headquarters at Mount Abu, Rajasthan, India and in
other countries. In this form of meditation the
individual sits in a relaxed & comfortable position
with their eyes open, and with gaze fixed on a
meaningful symbol (a light) & then uses visual or
auditory images for concentration (6). At the same
time they actively think positive thoughts about a
Universal force pervading all over, as light and peace
(7). This study was carried out to address the lack
of research on Rajyoga meditation specifically. The
objective of this study was to assess the effect of
Rajyoga meditation in patients of CTTH, using Visual
Analogue Scale (VAS), a patient’s subjective,
numerical assessment of pain intensity. |
The present study was conducted on 50 subjects, 18-58 years, undergoing treatment for CTTH in the department of Psychiatry in Sri Guru Ram Das Institute of Medical Sciences & Research, Amritsar. The protocol of study was approved by the ethical committee of our institute. Patients were informed about the methodology of the project and the need for regular follow up was emphasized. CTTH was diagnosed by the criteria laid down by the International Headache Society for Chronic Tension Headache (8). The inclusion criteria was the presence of primary headache with duration more than 4 hrs a day and frequency of 15 or more days monthly for at least 6 months. Patients with headache for less than 6 months were excluded. Patients with headache due to sinusitis, eyestrain, cervical spondylosis, posttraumatic headaches and severe depression were also excluded from the study. All those patients who could not come for regular training of Rajyoga meditation were also excluded. The patients who did not volunteer for meditation were taken as controls. The subjects were divided into 2 groups. Group 1 (study group) subjects were taught relaxation therapy in the form of Rajyoga meditation in the psychiatry department. Group 2 were controls. The patients were monitored for 8 weeks and subsequently analysed using Visual Analogue Scale. This was a prospective randomized, single blindstudy. Rajyoga meditation was taught to study group by the author herself who is a Brahmakumari and is associated with Prajapita Brahmakumari Ashram, Amritsar for the last 20 years. Meditation was done in a silent dimly lit room. Meditation was taught to subjects in batches of 3-4 subjects per batch, between 10-1 pm. Group Meditation training was given with the help of pictures, diagrams and audio cassettes. A total of 8 lessons each of 45 minutes were given. 25 minutes were devoted to instruct them on the meditation technique and 20 minutes for performing meditation with guided commentary. Meditation was presented with the suggestion that this technique is powerful and regular practice can bring relief from pain in many cases. In this way a positive placebo effect was maximized. The patients were also instructed to perform meditation in a similar manner for 20 minutes each day at home. They were also given Brahmakumari’s literature on positive thinking. Such material strengthened the belief that meditation can have significant physiological effects. In addition analgesics and muscle relaxants were also advised as per the psychiatrist's prescription. All the patients were required to note about meditation practice in their daily diary. Eight such sessions, twice a week, for 4 weeks were given followed by once a week interview for next 4 weeks during which the method followed by the patients was checked and any queries relating to the methodology were answered. At this time patient's compliance to practice of meditation was also tested (5). Controls were given analgesics and muscle relaxants only but no meditation was taught. Similar drugs and regimen was followed in both the groups. They were called once a week for 8 weeks and compliance about treatment was noted. Parameters measured were headache severity using VAS scale, frequency of headache per week and duration of each episode. All the subjects were required to write in their diary the following parameters i.e. severity of headache on VAS Scale (scale 0 as no pain and 10 as maximum pain), frequency of headache per week, duration of each headache episode in hours and regularity of medication intake. Study group patients in addition also noted the duration and timing of meditation. Headache index was calculated by multiplying severity of headache and frequency of headache per week. Statistical analysis For quantitative variables such as headache severity, frequency duration and headache index, summary statistics as mean and standard deviation were calculated for both groups separately. The basal values for all the quantitative parameters between the two groups were compared using Student 't' test. P values detected smaller than 0.05 were considered as significant. The extent of relief in headache in both groups at the end of 8 weeks was calculated in percentage and tabulated. |
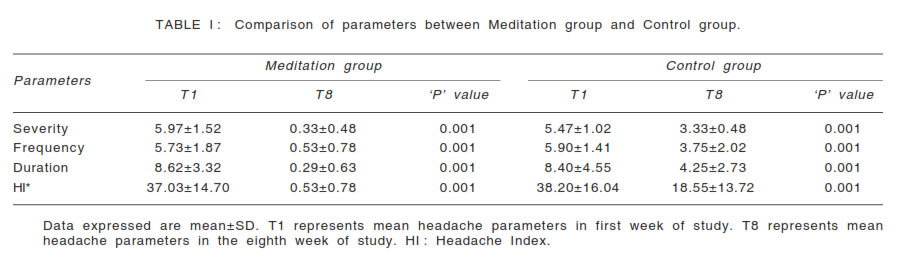
Seventy patients entered the study, 35 in Group 1 (study group) and 35 in Group 2 (control group). Eight patients were lost to follow up after the first treatment period had commenced and also ignored subsequent correspondence. There was a further withdrawal of 12 patients during the subsequent 8 weeks, some due to inability to continue meditation and some due to non compliance of treatment and follow up. By the end of 8 weeks we had data of 30 patients in the study group and 20 in the control group. On comparing the demographic profile of the patients in two groups we found that they were comparable regarding age, sex, social status and marital status to those in control group. The age of the patients ranged from 18-58 years. Mean age of the patients was 32.06+9.43. The male is to female ratio was 11:39. The duration of headache was ranging from 6 months to 6 years and the mean duration of the headache was 2.06+1.53. There were more females than males and more married people than unmarried ones in both the groups. The parameters between meditation and control group are compared in Table I. Severity of headache as assessed by VAS scale showed highly significant reduction in severity of pain (p<0.001) in Group 1. The percentage relief of headache was 94% after 8 weeks. The control group also showed highly significant improvement in severity of headache with medication alone but the percentage of improvement after 8 weeks was merely 36%. Percentage relief in frequency of headache was 91% in study group as compared to controls (36%). 97% improvement in duration of headache was observed in study group, in comparison to just 49% in controls. Mean headache relief as calculated by Headache index (severity of headache multiplied by frequency of headache per week) was 99% in subjects practising meditation, whereas it is almost half (51%) in the control group. The most striking observation was that most of the
patients experienced considerable improvement in the
condition over the course of 8 weeks of their training
program of Rajyoga meditation. There improvement
was highly significant (p<0.001) in all the parameters
at the end of 4 weeks in study group whereas the
control group showed improvement only after 6-8
weeks. The mean value of the severity of headache
dropped highly significantly during the first 4 weeks
of meditation practise in study group (p<0.001) as
compared to control group (p=0.008). Similar trend |
 |
This study attempts to compare the influence of
Rajyoga meditation on CTTH patients on regular
medication. Meditation is believed to gradually reduce
sympathetic dominance resulting in better balance
between sympathetic and parasympathetic. Studies
have proven that regular practice of Rajyoga
meditation increase self satisfaction by enhancing
positive thinking (10), decreases heart rate and blood
pressure (11), and has cardio-protective effect (12). Meditation helps the patient to change his way of looking at situations and people. He learns how to gain liberation from circumstances. This approach is recognized in modern psychology as 'cognitive reappraisal'. Moreover, meditation is said to release endorphins from brain which are better pain killers than pills or injections. (15). Since Rajyoga meditation is related mainly to mind and one is required to stop only worldly and negative thoughts and concentrate the mind on God, it is quite possible that the relief in symptoms of study group of was due to effect on supraspinal levels mainly the limbic system and is known to modulate the endogenous pain control system. Meditation and yogic asanas involve and influence various neural sites involved in sensory imagery mainly hippocampus and higher order association regions and executive systems i:e dorsolateral prefrontal cortex, anterior cingulate gyrus, striatum, thalamus, pons, and cerebellum (16) respectively The results of this study effectively demonstrates the role of Rajyoga meditation in early and quick relief of CTTH if practised regularly, along with the medical treatment. This study also strengthens the efficacy of psychological approaches in the management of chronic pain including chronic headaches. Conclusion In conclusion, Rajyoga meditation has stood the test of time and is relevant today in management of myriad illnesses as well as for research into states of consciousness. We suggest that physicians consider offering this meditation training as an alternative to suitable headache patients. Once learnt, the practice involves no financial expense to the patient. The limitations of this study were, firstly the sample sizes for the study and control group were small and the assessment was done after a short duration of time which limited the statistical power and reliability of effect size estimates. Further progressive studies should be conducted on larger group and over a longer time period. Secondly only one measure of pain i.e. VAS scale was used. Use of multidimensional pain assessment tools that assess the sensory and affective dimensions of pain will benefit future studies. |
|